The Cultural Stigma Around Mental Health
3 Aralık 2022")
Khudeeja Dawar
According to the World health organization in Cultural Perspectives on Mental Health, n.d estimated that 20% of the world’s population suffers from mental illness at some point in their life. Keeping this estimate in mind, 1 out of 5 people and a total of one billion people in the world suffer from mental illness. Resulting in everyone knowing someone suffering from mental disorders. The fact that many of us may think that we do not is mainly because of the inconvenient truth that is a high stigma around mental health. Cultural norms and religious beliefs often influence the origin of mental illness, and also the stigma that surrounds it (Cultural Perspectives on Mental Health, n.d.) The word stigma is defined as dishonor and disgrace. The stigma around mental health is a universal phenomenon (Gaebel et al., 2016, p. 67), but it is socially constructed. In this context, this research paper will illustrate how the element of time and culture influence the taboo around mental health.
People who are suffering from mental health problems and other disorders are the people who have been the most pilloried, underprivileged, and vulnerable to discrimination in our society (Johnstone, 2001, p. 201). According to the world health organization in 2001, stigma and discrimination declared it to be the single most important barrier we require to overcome in this society (Cultural Perspectives on Mental Health, n.d.). There is a misconception that a mental health issue is an individual problem. Andrade (2017) argues that it is caused due to a combination of biological, genetic, and cultural factors. The cultural factor plays an important role in making mental health issues a general problem (Andrade, 2017). Often culture and background are ignored as a factor, causing mental illnesses and also the stigma which surrounds it which enables people to openly talk about it. People because of the stigma forestall seeking professional help just to avoid labels (Downey et al., 2012).
Stigma causes disadvantages on an individual level as well as on a structural level (Gaebel et al., 2016, p. 86). The study by Downey et al. (2012) on patients in an ER is altogether an incredible study to show individual-level disadvantages due to the stigma. The study concluded that 45% of an opportunity sample that entered a specific ER for non-psychological reasons, tested positive for an undiagnosed mental illness, such as depression, and general anxiety disorder. There is no disagreement that the stigma is affecting people on a structural level, such as the care-taking unit which is highly affected due to the stigma that is blocking the recovery process for the patients’ treatment (Delaney, 2012, pp. 333-334). The stigma around mental health is affecting the medical field making them incompetent to perform their vital role which is affecting the patient’s well-being as the nurses are not providing the proper care and treatment which is required. According to Delaney (2012, p. 333), the nurses are aware of the stigma, but they are not letting themselves see which explains perfectly the way the stigma alters our behavior. Stigma is not only affecting the practicing nurses but also the trained clinicians, as they are also affected by the stereotyping of mental health. They also reflect attitudes and discriminatory practices (General, 2001). This is the main reason why a person with mental illness, rather than seeking help ignores it till it gets worst.
The main reason for stigma construction is social behaviors. Social behavior can be explained as how people respond to certain situations that influence or be influenced by others living in the same society. As society plays a vital role in stigma formation, it is noted that it happens mainly due to the reason which is the gap between the general perception of mental disorders, and what they really are. This lack of knowledge in people is said to be the root problem of stigmatization (Hinshaw, 2009). A study by Gilbert et al., (2007) tried to illustrate how the rate of the stigma around mental health differs in different age groups. The results stated that people in the age group of 55 and above have a noticeably high rate of stigma around mental health than in the age group below 55. The main reason was concluded to be the lack of acceptance and knowledge. This actively demonstrates that people with an age above 55 have less capacity to accept new perspectives towards different topics. They are well-rooted towards their old traditional beliefs and show a high degree of unacceptance towards unlike viewpoints. In addition to this, they don’t want their future generations to detract either, consequently, their beliefs are passed down as family heritage causing stigma. The correct knowledge about these topics is unaccepted by them for example in earlier times people used to confuse mental illness with witchcraft (Rastogi et al., 2014, p. 16) and still do in many cultures. This shows the unwillingness to accept and creates a gap in knowledge. The lack of information is one of the initial reasons behind the stigma formation which leads to negative labels. (Abdullah & Brown, 2011). The lack of correct knowledge and not accepting new perspectives on these complex topics leads to societal stereotyping. These negative stereotypes are very harmful and damaging to a person’s self-esteem, who is experiencing these types of symptoms. For example, in India, a person who has any degree of mental disorder is considered to be deranged (Rastogi et al., 2014, p. 16). Stigma, in other words, is the fear of not being accepted in society. Negative labels and attitudes cause masses to develop emotions such as horror, abandonment, and also discrimination against the person suffering from mental disorders (Corrigan & Penn, 1999).
These negative labels of society give birth to three types of stigma: Self, Courtesy, and Structural stigma. Self-stigmatizing refers to the internal feeling of guilt, shame, and an inferior mindset which is shaped by society for the individual (Heather Stuart, 2005). The step of self-stigma development consists of awareness of the negative stereotypes of society, agreeing with the stigma, and applying it to themselves (Gaebel et al., 2016, pp. 50- 52). This makes an individual to restrict himself to seek treatment just to avoid labels and limit themselves in society only for society to accept him(Cultural Perspectives on Mental Health, n.d.). The other type of stigma formed by societal views is courtesy. Goffman in 1963 coined the term courtesy stigma (Gaebel et al., 2016). The courtesy stigma or in other words, the stigma by association means how people in a society judge and label people who are suffering from mental illnesses to determine that they do not fit the social norms (Overton & Medina, 2008, p. 148). The earliest stages which can develop into mental illness, such as expressing emotional pain through crying or raising their voice are often negatively taken and they are shunned rather than encouraged to seek help. This type of stigma, fear of not being accepted, around mental health is one of the main factors that enables the person to seek help until it is dangerous to the person himself or others. The third type is Structural stigma which is very much similar to the courtesy stigma. It deals with how structural-level policies intentionally or unintentionally are restricting the opportunities of a mental health individual based on negative stereotyping (Gaebel et al., 2016, p. 53). According to Johnstone (2001), half of all states in the USA prohibit child custody rights for a person having any mental health history. Another example of this is that in some USA states a person with ongoing treatment or any history is ineligible to vote or have any holding in public offices. This shows that the negative stereotypes of society form the stigma which is the root cause of the taboo often attached to people suffering from mental illnesses.
In the Middle Ages, the opinions of people were restricted due to the absence of technology and exposure to different standpoints of people at that time but today as we live in a modern era with access to the internet where people can have an insight into various topics easily. However, there is very little change in the thinking mindset of people today compared to earlier times. The Middle Ages are said to be the origin of the traditional beliefs which are passed on to generations. People at that time didn’t use to consider mental illness as an illness. In some cultures according to Stuart et al. (2012) people who experience symptoms such as hallucinating were considered to be noble and highly respected and also viewed as honored enough to hear god voices. However, in some cultures, it was considered as practicing witchcraft and was given the punishment of death (Julian & Warner, 2006). Not only this, Hinshaw Stephen P. (2009) in his book the mark of shame: the stigma of mental illness and an agenda for change states that the early human skulls were found displaying proof of round holes embedded in them. Skulls were pierced with a sharp spherical instrument. It was concluded that possibly this act was done to aid the people from evil spirits from their heads. This inhuman act is nothing but the stigma which began many centuries before, but today according to Hinshaw (2009) the modern beliefs of the stigma are compared to be the same but different. Beliefs are said to be different because of the new scientific discoveries, people started to believe mental health is separate from physical health but still tend not to accept it just to avoid labels. In early times, people used to distance themselves from the person suffering from mental illness, it is currently the same. The irony is that before people used to kill the person suffering from mental illness, but now discrimination, isolation, and unacceptance of that person in society drive that person to kill himself rather than the other way around. As we are living in the modern era, and still are not able to grow out of our old traditional beliefs. According to a study by Thompson et al. (2002) on a focused group of 7 Australian participants done through 129 in-depth interviews. The results were that stigma is associated with weakness of personality. Another study by Knifton et al. (2012) on 87 participants having Indian, Chinese and Pakistani backgrounds. The results state that Indian and Chinese participants were found to link mental illness with karma and some were found to link mental health with punishment from the god or caused due to jin or spirits. This proves that the way of thinking hasn’t changed that much and the reason behind this is the fact that these topics are not openly discussed.
Stigma is a universal problem (Cultural Perspectives on Mental Health, n.d.). People who are suffering from mental illnesses are viewed differently than people with physical illnesses (Julian & Warner, 2006) and at least once in their lifetime people with mental illnesses are accused of faking their symptoms. Viewing people with mental illness differently and blaming them for their condition is like blaming a person for getting a fever. It’s neither the person’s fault nor their choice to have mental illness in their lives, but the stigma surrounding mental illness is leading to discrimination which is a huge barrier for people who are suffering to seek treatment and live a quality of life. The culture is affecting the construction of the stigma. The stigma is present in all cultures, but in some places, it has a greater impact than in others. In a survey of 16 countries in the Americas, Middle East, Africa, Europe, Asia, and South Pacific. The results displayed that 22.1% and 11.7% of participants from developing countries and developed countries showed signs of embarrassment and discrimination because of mental illnesses. This survey perfectly shows how different cultures enhance the stigma. In a study done to demonstrate the difference between the stigma of different cultures, Weiss et al. (2001) took two sample groups one from Bangalore and the other from London. Both groups were asked questions related to mental illness and its consequences. The Bangalore sample showed signs of concerns related to a good marriage. However, the London sample showed no concern for marriage, but the London sample was found to have a higher rate of self-stigmatizing than the Bangalore sample. Just like London displays a higher rate of self-stigma, China is considered to have the highest rate of courtesy stigma because of its strong family lineage (Yang et al., 2007). These studies perfectly demonstrate the universality of stigma and how culture influences the changes in stigma.
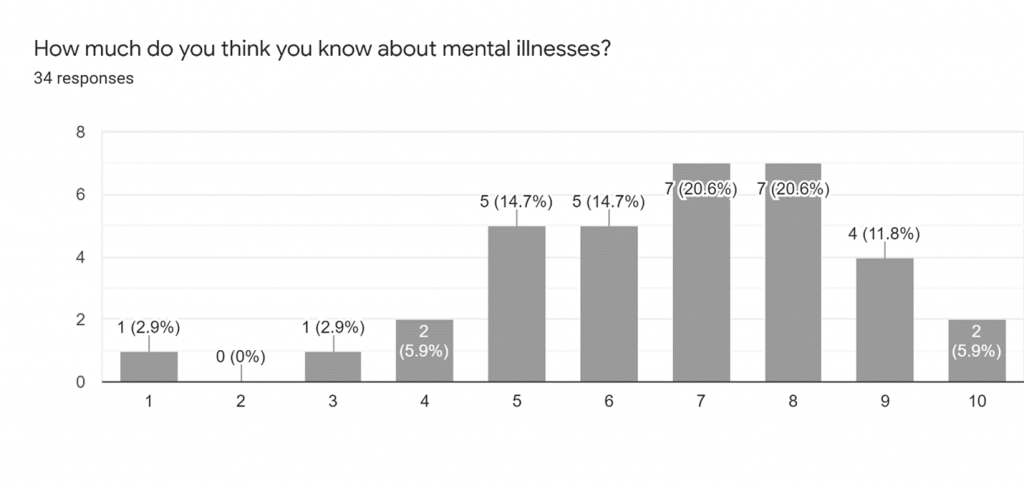
I conducted a questionnaire survey to further support my argument made above. Respondents to the survey were asked to answer a total of 5 questions with no mention of the word “stigma” to get accurate and honest views they hold about mental illnesses. The aim of the survey for research purposes is to help prove and display the gap of knowledge as mentioned in the claims made above and the general view to show the presence of the stigma in their thinking. Two of the questions in the survey help in identifying the presence of the stigma in their thinking as being direct or indirect. The limitation of the survey is that the age group is mainly between 19-23 and all of the respondents have a student qualification. This survey could be more accurate if done on different age groups. The total number of responses collected is 34. The first question (see Appendix for the question) asked was to identify the presence of the indirect stigma which we all are affected by one way or another. In response to this question, 91.2% of responses were yes, 2.9% were no and 5.9% were maybe. This demonstrates that people not having accurate knowledge about the symptoms and make assumptions limited to their own thinking which leads to negative stereotyping as mentioned above. The second question (see Appendix for the question) asked in the survey also shows the presence of stigma. From four options Headache, Depression, Back pain, Panic attack. 90.9% of the respondents answered headache and 9.1% answered back pain. 0.0% for depression and panic attacks support the claim made by Julian and Warner (2006) in his journal article about mental illness being viewed differently than physical illness, which is also mentioned above. This proves that in society mental illnesses are not taken into account to have the same damaging effect as any physical illness. In addition to this, we also come to understand that a person living in a stigmatized society tries to hind their mental illness behind any physical illness just to avoid the judgment of people (negative stereotyping) and discrimination that the person will receive. The 4th and 5th questions (see Appendix for the questions) exhibited positive answers toward mental health and also expressed a willingness to help. The answer to the last question (see Appendix for the question) is the reason behind the positive responses to the 4th and 5th questions. Most of the people scaled their knowledge about mental illness between 6-8. As the majority of the respondent were students, having exposure to a different point of view through social media or academia increased their acceptance to help.
Culture plays an important role in establishing the stigma around mental health. People have many misconceptions of what encompasses a mental disorder and are often unaware of the severity of the effects a mental illness stigma can have on your thinking process and in turn, the way you behave with the people around you. Cultural norms and religious beliefs often influence the origin of mental illness, and also the taboo that surrounds it (Cultural Perspectives on Mental Health, n.d.). And the formation of the stigma is very much influenced by societal norms. It is caused due to the lack of knowledge and unacceptance of new understanding. This causes negative stereotyping in society which gives birth to 3 types of stigma. With time the stigma leads to discrimination which is a huge barrier for people suffering from mental issues to seek treatment and live a quality life. But in some cultures, the rate of stigma is higher than the others which also affects a person’s willingness to seek treatment in society which harms their quality of life.
References
- Abdullah, T., & Brown, T. L. (2011). Mental illness stigma and ethnocultural beliefs, values, and norms: An integrative review. Clinical Psychology Review, 31(6), 934–948. https://doi.org/10.1016/j.cpr.2011.05.003
- Andrade, S. (2017, May 16). Cultural Influences on Mental Health. The Public Health Advocate. https://pha.berkeley.edu/2017/04/16/cultural-influences-on-mental-health/
- Cultural Perspectives on Mental Health. (n.d.). Unite For Sight. https://www.uniteforsight.org/mental-health/module7
- Delaney, K. R. (2012). Psychiatric Mental Health Nurses: Stigma Issues We Fail to See. Archives of Psychiatric Nursing, 26(4), 333–335. https://doi.org/10.1016/j.apnu.2012.04.006
- Downey, L., Zun, L., & Burke, T. (2012). Undiagnosed Mental Illness in the Emergency Department. The Journal of Emergency Medicine, 43(5), 876–882. https://doi.org/10.1016/j.jemermed.2011.06.055
- Gaebel, W., Sartorius, N., & Rössler, W. (Eds.). (2016, August 10). The Stigma of Mental Illness – End of the Story? Springer, Cham. https://doi.org/10.1007/978-3-319-27839-1
- General, O. O. T. S. (2001, August). Chapter 1. Introduction – Mental Health: Culture, Race, and Ethnicity – NCBI Bookshelf. The National Center for Biotechnology Information. https://www.ncbi.nlm.nih.gov/books/NBK44246/#
- Gilbert, P., Bhundia, R., Mitra, R., McEwan, K., Irons, C., & Sanghera, J. (2007). Cultural differences in shame-focused attitudes towards mental health problems in Asian and Non-Asian student women. Mental Health, Religion & Culture, 10(2), 127–141. https://doi.org/10.1080/13694670500415124
- Hinshaw, S. P. (2009). The Mark of Shame: Stigma of Mental Illness and an Agenda for Change (1st ed.). Oxford University Press.
- Hsin Yang, L., Thornicroft, G., Alvarado, R., & Vega, E. (2014). Recent advances in cross-cultural measurement in psychiatric epidemiology: utilizing “what matters most” to identify culture-specific aspects of stigma. International Journal of Epidemiology, 43(2). https://doi.org/10.1093/ije/dyu039
- Johnstone, M. J. (2001). Stigma, social justice and the rights of the mentally ill: Challenging the status quo. Australian and New Zealand Journal of Mental Health Nursing, 10, 200–209.
- Julian, L. & Warner, R. (2006). Social Inclusion of People with Mental Illness. Cambridge University Press.
- Overton, S. L., & Medina, S. L. (2008). The Stigma of Mental Illness. Journal of Counseling & Development, 86(2), 143–151. https://doi.org/10.1002/j.1556-6678.2008.tb00491.x
- Rastogi, P., Khushalani, S., Dhawan, S., Goga, J., Hemanth, N., Kosi, R., Sharma, R. K., Black, B. S., Jayaram, G., & Rao, V. (2014). Understanding clinician perception of common presentations in South Asians seeking mental health treatment and determining barriers and facilitators to treatment. Asian Journal of Psychiatry, 7, 15–21. https://doi.org/10.1016/j.ajp.2013.09.005
Appendix
| Questions | Option 1 | Option 2 | Option 3 | Option 4 | |
|---|---|---|---|---|---|
| 1. Have you ever addressed someone with words like Lazy, Rude, Crazy, or Mad? | YES= 91.2% | NO= 2.9% | MAYBE= 5.9% | ||
| 2. if you want to make an excuse for not attending a meeting? Which option will you choose? | Headache= 90.9% | Depression= 0.0% | Back pain= 9.1% | Panic attack= 0.0% | |
| 3. would you hire or work with a person suffering from mental illness? | 3. would you hire or work with a person suffering from mental illness? | YES= 38.2% | NO= 17.6% | NO= 17.6% | MAYBE= 44.1% |
| 4. how would you react if someone you know is diagnosed with mental illness | stay away= 5.9% | help them= 91.2% | Communication= 5.9% | ||
| 5. How much do you think you know about mental illnesses? | (See the graph on the next page) |